












- By FYH News Team
[ad_1]
Missed scheduled clinic appointments (ie, no-shows) are more common among uninsured patients from racial and ethnic minority groups living in economically disadvantaged areas and contribute to poorer health outcomes.1–3 In the pediatric population, the implications of telemedicine for no-show rates have not been adequately explored despite the widespread adoption of telemedicine during the COVID-19 pandemic. The aim of this study was to ascertain whether patient race and ethnicity and level of socioeconomic disadvantage were associated with no-show rates for in-person and telemedicine clinic visits.
This retrospective comparative effectiveness study involved outpatient visit data from a multisite comprehensive pediatric gastroenterology practice. Visits were divided into 2 groups delimited by the March 2020 Centers for Medicare and Medicaid Services telehealth expansion. The in-person group included all in-person clinic visits from March 1, 2016, to February 29, 2020, when only in-person visits were scheduled; the telemedicine group included all telemedicine visits from April 1, 2020, to August 1, 2021, when telemedicine visits predominated. March 2020 visits were excluded to allow for a 1-month interim washout period. The Boston Children’s Hospital Institutional Review Board approved the study and waived the requirement for informed consent because of minimal patient risk. The study followed the ISPOR reporting guideline.
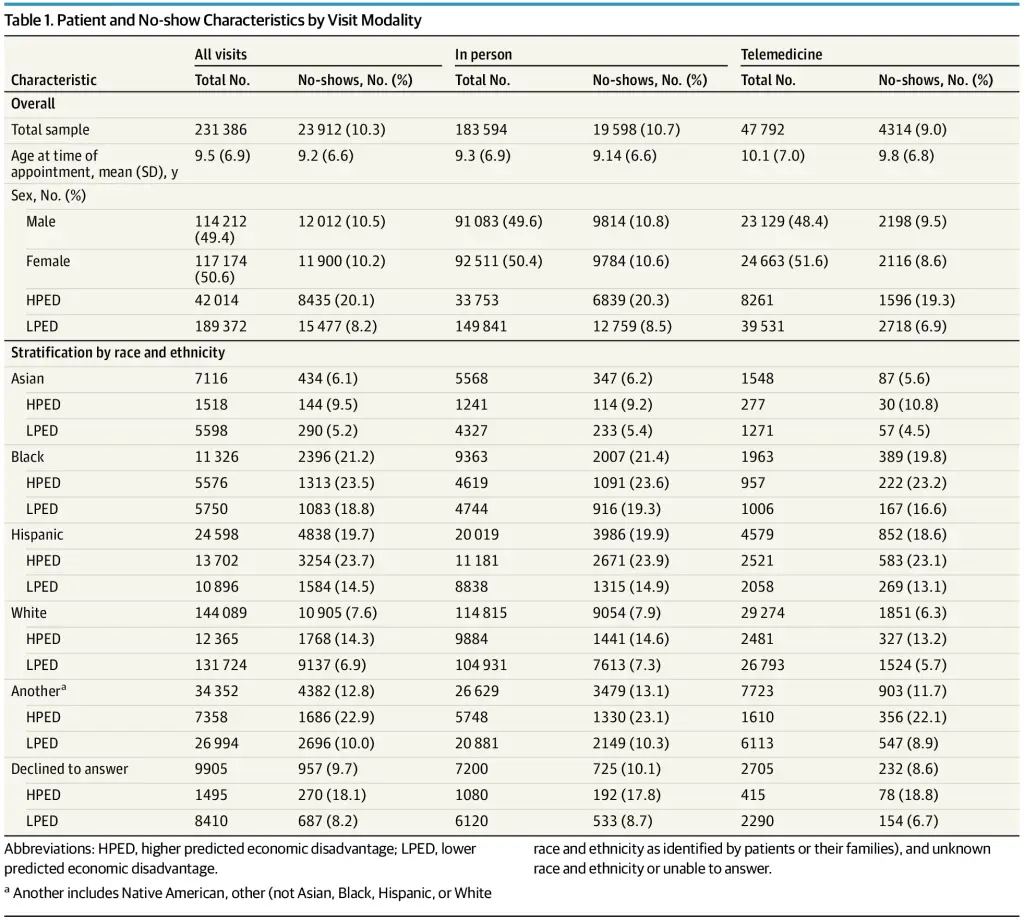
Patients resided in Massachusetts and were classified as having a higher probability of economic disadvantage (HPED) or lower probability of economic disadvantage (LPED), a binary latent variable for income status. Patients with HPED used public health insurance and resided within one of the top 25% highest poverty rate zip codes in Massachusetts.4 Patients not meeting both criteria were classified as LPED. Nonoverlapping primary race and ethnicity were selected by patients or their families during registration and aggregated into the following categories: Asian, Hispanic, non-Hispanic Black, non-Hispanic White, declined to answer, or another (Native American, other [not Asian, Black, Hispanic, or White race and ethnicity], and unknown or unable to answer).
For each comparison, a hierarchical generalized linear mixed model was constructed and adjusted for random effects among multiple encounters by the same patient, incorporating age at visit, sex, distance traveled to the clinic, and income status as independent variables. Models used a binomial distribution and logit link function to account for binary outcomes. Resulting fixed-effects estimates were exponentiated to generate adjusted odds ratios, with P < .05 considered significant. Stata, version 17.0 was used.
Of 231 386 visits, 183 594 constituted the in-person group, and 47 792 constituted the telemedicine group (Table 1). For all visits combined, HPED status was associated with higher no-show odds (adjusted odds ratio [aOR], 4.03; 95% CI, 3.83-4.24; P < .001), a consistent finding across all racial and ethnic groups (Table 2). Higher probability of economic disadvantage was associated with higher no-show odds for telemedicine visits vs in-person visits (aOR, 4.99; 95% CI, 4.44-5.61; P < .001 vs 3.86; 95% CI, 3.66-4.08; P < .001), an observation consistent across all racial and ethnic groups (Table 2). Controlling for sex and age, telemedicine was associated with lower no-show odds only for LPED patient visits (aOR, 0.85; 95% CI, 0.81-0.90; P < .001 vs HPED aOR, 1.04; 95% CI, 0.96-1.12; P = .35).
We found that differences in clinic no-show rates are associated with a patient’s level of economic disadvantage. The finding that telemedicine was associated with an overall improvement in clinic attendance supports previous studies; however, this improvement was not observed in visits for patients with HPED.5,6 This lack of improvement may reflect the disproportionate COVID-19 pandemic–related stressors experienced by families using public health insurance and residing in communities with higher poverty rates.
Limitations of this study include unmeasured confounders influencing clinic attendance (ie, severity of symptoms and diagnosis); the lack of individually validated patient statuses for LPED or HPED; and the unexamined generalizability to other subspecialties. However, as telemedicine continues to shape the clinical encounter landscape, these findings show that efforts are needed to ensure that all patients receive equitable care.
Accepted for Publication: January 26, 2022.
Published Online: May 23, 2022. doi:10.1001/jamapediatrics.2022.1510
Corresponding Author: McGreggor Crowley, MD, Division of Gastroenterology, Hepatology, and Nutrition, Boston Children’s Hospital, 300 Longwood Ave, Boston, MA 02115 (paul.crowley@childrens.harvard.edu).
Author Contributions: Mr Brociner and Dr Crowley had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Brociner, Yu, Crowley.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: Brociner, Crowley.
Critical revision of the manuscript for important intellectual content: All authors.
Statistical analysis: Brociner, Yu, Crowley.
Obtained funding: Crowley.
Administrative, technical, or material support: Yu, Crowley.
Supervision: Kohane, Crowley.
Conflict of Interest Disclosures: Dr Yu reported receiving grants from the National Institutes of Health National Institute of General Medical Sciences and being an inventor of US patent 16/179,101, that is, quantitative pathology analysis and diagnosis using neural networks, assigned to Harvard University outside the submitted work. No other disclosures were reported.
SC, Marcin
JP, Dayal
P, Tancredi
DJ, Crossen
S. Impact of telemedicine on visit attendance for paediatric patients receiving endocrinology specialty care. J Telemed Telecare. 2020;X20972911. Published online November 23, 2020. doi:10.1177/1357633X20972911PubMedGoogle ScholarCrossref
[ad_2]
Source link
Trending Topics

Features
- Drive Toolkit
Download and distribute powerful vaccination QI resources for your community.
- Health Champions
Sign up now to support health equity and sustainable health outcomes in your community.
- Cancer Early Detection
MCED tests use a simple blood draw to screen for many kinds of cancer at once.
- PR
FYHN is a bridge connecting health information providers to BIPOC communities in a trusted environment.
- Medicare
Discover an honest look at our Medicare system.
- Alliance for Representative Clinical Trials
ARC was launched to create a network of community clinicians to diversify and bring clinical trials to communities of color and other communities that have been underrepresented.
- Reducing Patient Risk
The single most important purpose of our healthcare system is to reduce patient risk for an acute event.
- Jessica Wilson
- Victor Mejia
- Subash Kafle



