










- By FYH News Team
[ad_1]
During the COVID-19 pandemic, use of digital technology has become more widespread for routine activities for children (eg, medical visits, remote learning), perpetuating concerns about the US socioeconomic “digital divide.”1 In 2021, 19.7% of parents reported using telemedicine for their child.2 However, for health care to adequately address children’s health needs, defining the quality, access, and use of digital technology among families is essential. We characterize the type and quality of digital access among racially and ethnically as well as socioeconomically diverse households in Chicago and the associations with child and household characteristics.
Data collection for this cross-sectional study occurred from May 24 to July 29, 2021, through a panel survey of parents in English and Spanish via web and telephone. Eligibility criteria included being 18 years or older, the parent of at least 1 child living in the household, and a Chicago resident. Respondents were recruited from probability samples (1134 of 2280 eligible responses [49.7%]) (eMethods in the Supplement). The institutional review board at Lurie Children’s Hospital approved the study, and participants provided electronic consent. This study followed the STROBE reporting guideline.
Survey questions addressed type of device, perceived internet speed, internet costs, and concerns about affordability (eTable in the Supplement). Demographic characteristics and child health status were collected. Self-reported parent race and ethnicity were categorized as Asian and other race or ethnicity (which were combined owing to small sample size), Hispanic or Latinx, non-Hispanic Black (hereinafter Black), and non-Hispanic White (hereinafter White). All percentages and analyses were population weighted; a 2-sided P < .05 was considered significant. Differences in digital access by child health status and demographic characteristics were examined using χ2 tests. Analyses were performed in SAS software, version 9.4 (SAS Institute, Inc). Multivariable logistic regression examined the likelihood of having high-speed internet with race and ethnicity and household income as covariates.
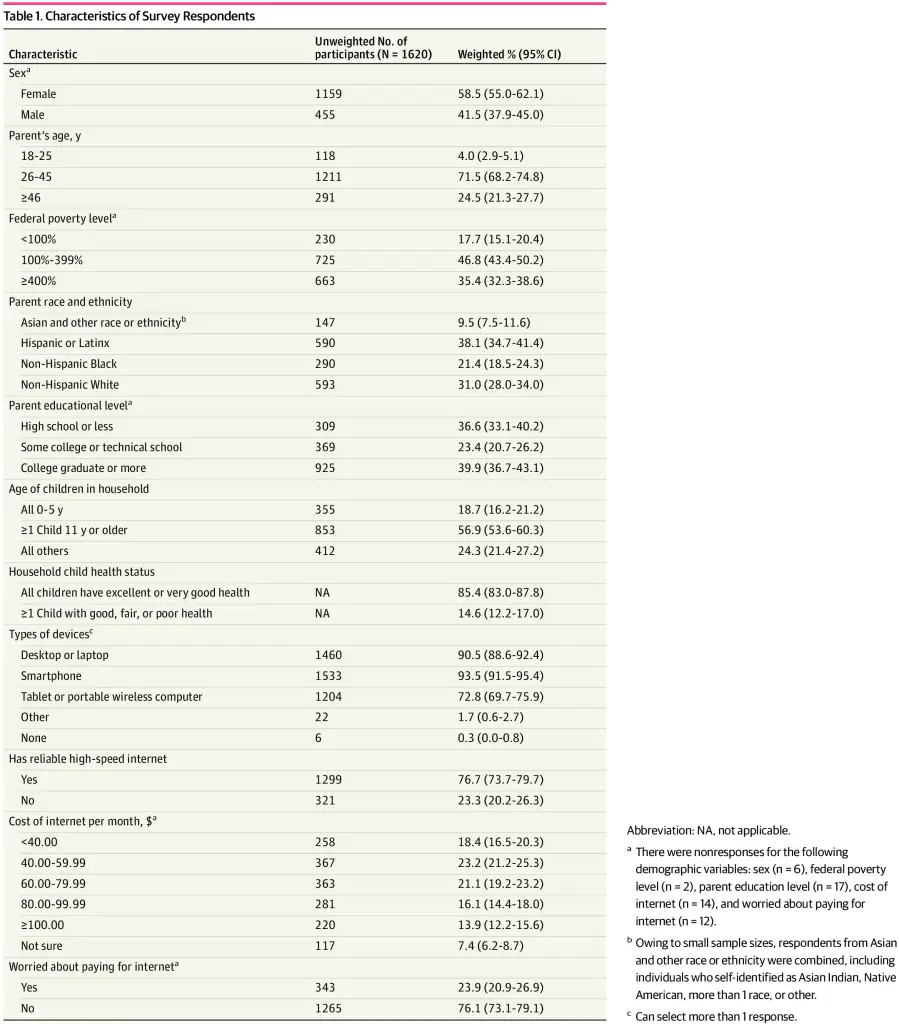
Data from 1620 Chicago parents (58.5% [95% CI, 55.0%-62.1%] women and 41.5% [95% CI, 37.9%-45.0%] men; 71.5% [95% CI, 68.2%-74.8%] aged 26-45 years) were collected. In terms of race and ethnicity, 9.5% (95% CI, 7.5%-11.6%) were Asian or other, 38.1% (95% CI, 34.7%-41.4%) were Hispanic or Latinx, 21.4% (95% CI, 18.5%-24.3%) were Black, and 31.0% (95% CI, 28.0%-34.0%) were White. Most parents (90.5% [95% CI, 88.6%-92.4%]) reported having a desktop or laptop at home, and 76.7% (95% CI, 73.7%-79.7%) reported having reliable high-speed internet (Table 1). Black and Hispanic or Latinx parents were less likely to have reliable, high-speed internet (76.0% [95% CI, 69.5%-82.6%] and 64.5% [95% CI, 58.8%-70.2%], respectively) vs White parents (88.8% [95% CI, 85.3%-92.3%]; P < .001) (Table 2). Child health status was not associated with having high-speed internet. In the multivariable model, Hispanic or Latinx parents were less likely to have high-speed internet vs White parents (odds ratio, 0.45 [95% CI, 0.28-0.73]) after controlling for household income. There was no significant difference for having high-speed internet between Black and White parents (odds ratio, 0.92 [95% CI, 0.53-1.61]).
The findings of this population-weighted cross-sectional survey of Chicago families suggest that disparities in digital access were associated with race and ethnicity as well as income but were not associated with child health status. After adjusting for income, the disparity in access to high-speed internet persisted for Hispanic or Latinx but not Black participants. This may be attributed to racial and ethnic residential segregation, because Chicago ranks high nationally on segregation indices, suggesting that broadband services may be limited in neighborhoods with residents who are members of racial or ethnic minority groups.3 Previous studies have found that Hispanic or Latinx adults are more likely than Black or White adults to report having smartphone internet only.4 Barriers to access might include affordability and real or perceived low demand, discouraging internet carriers to invest in broadband infrastructure where Hispanic/Latinx families live.5
Study limitations include the generalizability to a national population, participants’ representativeness by income of Chicago families, and possible underrepresentation of participants with limited internet access. These findings are important for the design and implementation of digital health services and policies in childrens’ health care, ensuring that specific populations are not overlooked.6
Accepted for Publication: July 13, 2022.
Published: August 26, 2022. doi:10.1001/jamanetworkopen.2022.28992
Open Access: This is an open access article distributed under the terms of the CC-BY License. © 2022 Kan K et al. JAMA Network Open.
Corresponding Author: Kristin Kan, MD, MPH, MSc, Division of Advanced General Pediatrics and Primary Care, Department of Pediatrics, Ann & Robert H. Lurie Children’s Hospital of Chicago, 225 E Chicago Ave, Box 162, Chicago, IL 60611 (kkan@luriechildrens.org).
Author Contributions: Dr Heffernan had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Kan, Heard-Garris, Morales, Davis, Heffernan.
Acquisition, analysis, or interpretation of data: Kan, Bendelow, Lewis-Thames, Heffernan.
Drafting of the manuscript: Kan, Heard-Garris, Bendelow, Heffernan.
Critical revision of the manuscript for important intellectual content: Kan, Bendelow, Morales, Lewis-Thames, Davis, Heffernan.
Statistical analysis: Bendelow.
Administrative, technical, or material support: Kan, Morales, Lewis-Thames, Davis, Heffernan.
Supervision: Kan, Heffernan.
Conflict of Interest Disclosures: Dr Kan reported receiving grants from the Agency for Healthcare Research and Quality (AHRQ) during the conduct of the study. No other disclosures were reported.
Funding/Support: This study was supported by an anonymous family foundation and the Patrick M. Magoon Institute for Healthy Communities at Lurie Children’s Hospital for Voices of Child Health in Chicago (Dr Heffernan and Ms Bendelow); the AHRQ (Dr Kan); the National Heart Lung and Blood Institute (NHLBI) (Dr Heard-Garris); the National Cancer Institute (NCI) (Dr Lewis-Thames); Northwestern University Clinical and Translational Sciences Institute (Dr Lewis-Thames); Respiratory Health Association of Metropolitan Chicago (Dr Lewis-Thames); the National Institute on Aging (NIA) (Dr Lewis-Thames); and the Northwestern University Center for Community Health (Dr Lewis-Thames).
Role of the Funder/Sponsor: The sponsors had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclaimer: Dr Kan is an assistant editor of JAMA Network Open. She was not involved in any of the decisions regarding review of the manuscript or its acceptance. The content is solely the responsibility of the authors and does not necessarily represent the official views of AHRQ, NCI, NIA, NHLBI, or other listed funders.
Additional Contributions: Tracie Smith, MPH, supported this project as Director of Population Health Analytics in the Department of Data Analytics and Reporting at Lurie Children’s Hospital, for which she was not compensated.
C, Darville
G, Mercado
RE, Howell
S, Di Maggio
S. mHealth technology use and implications in historically underserved and minority populations in the United States: systematic literature review. JMIR Mhealth Uhealth. 2018;6(6):e128. doi:10.2196/mhealth.8383 PubMedGoogle ScholarCrossref
[ad_2]
Source link
Trending Topics
Features
- Drive Toolkit
Download and distribute powerful vaccination QI resources for your community.
- Health Champions
Sign up now to support health equity and sustainable health outcomes in your community.
- Cancer Early Detection
MCED tests use a simple blood draw to screen for many kinds of cancer at once.
- PR
FYHN is a bridge connecting health information providers to BIPOC communities in a trusted environment.
- Medicare
Discover an honest look at our Medicare system.
- Alliance for Representative Clinical Trials
ARC was launched to create a network of community clinicians to diversify and bring clinical trials to communities of color and other communities that have been underrepresented.
- Reducing Patient Risk
The single most important purpose of our healthcare system is to reduce patient risk for an acute event.
- Jessica Wilson
- Jessica Wilson
- Jessica Wilson




