August 23, 2022
4 min read
[ad_1]
August 23, 2022
4 min read
![]()
Disclosures:
A Conquer Cancer 2021 ASCO Registry Research Grant supported the study. Mullangi reports no relevant financial disclosures. Please see the study for all other authors’ relevant financial disclosures.
Certain patient demographics, including race and ethnicity and underlying primary malignant neoplasm, appeared associated with delays in cancer treatment among patients with COVID-19.
The findings, published in JAMA Network Open, showed some disparities in cancer care may have worsened during the COVID-19 pandemic.

The COVID-19 pandemic drastically affected oncologic care delivery, and the health care community recognized patients with cancer had a high susceptibility to infection, as well as severe complications and death, compared with those without a cancer diagnosis, Samyukta Mullangi, MD, MBA, hematology-oncology fellow at Memorial Sloan-Kettering Cancer Center, told Healio.

Samyukta Mullangi
“To that end, there were many professional and ad-hoc institutional guidelines about how to modify treatments to minimize infection risk, how frequently and in what contexts to screen patients for COVID-19, and what to do with a positive result,” Mullangi said. “We began to wonder whether these protocols, constructed with the best of intentions, may have led to unintentional harm by way of leading to delay in cancer treatments. As our thinking evolved and we received the data file from ASCO, we wanted to ask whether there were systemic differences between patients in their propensity to have a treatment delay. We hypothesized that among a cohort of patients who all tested positive for COVID-19, certain demographic factors would be associated with differential rates of delays in care.”
Investigators looked specifically for associations of factors such as race and ethnicity, social determinants of health, COVID-19 infection severity and timing of COVID-19 diagnosis with the risk for cancer treatment delays among 3,028 patients (49% aged 65 years or older; 58% women; 14% Black; 72% white; 10% Hispanic or Latino; 81% not Hispanic or Latino) who received treatment across 60 U.S. academic and community medical practices between March 2020 and July 2021 for a cancer diagnosis, and who also contracted COVID-19.
Researchers used multivariable analyses to assess delays more than 14 days between the originally planned date of cancer treatment initiation or discontinuation of cancer therapy.
Results showed 46% of patients experienced delays in cancer treatment or therapy discontinuation.
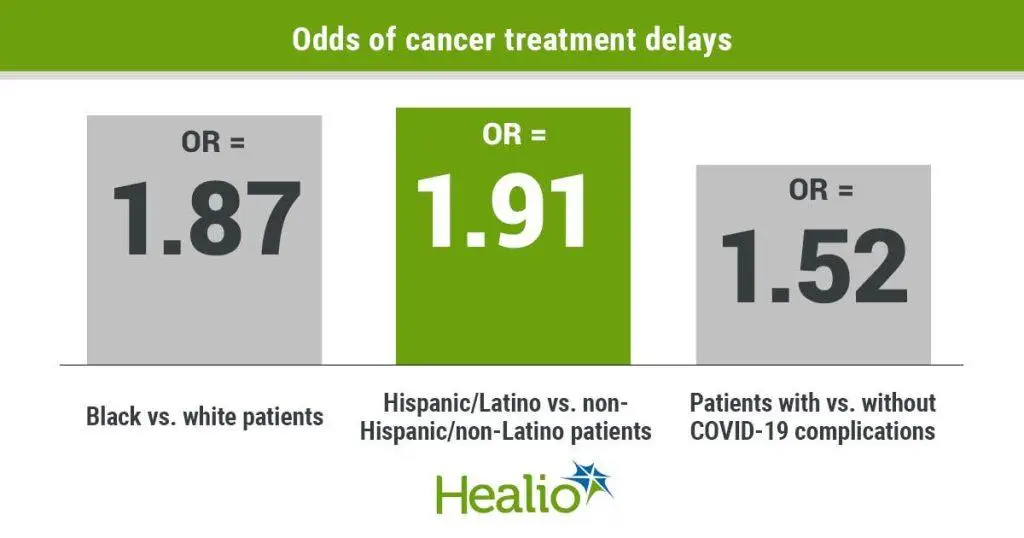
Researchers observed the highest rates of treatment delays among Black patients compared with white patients (OR = 1.87; 95% CI, 1.4-2.51), Hispanic or Latino patients vs. non-Hispanic or non-Latino patients (OR = 1.91; 95% CI, 1.34-2.72), patients with two or more comorbidities vs. patients with one or no comorbidities (OR = 1.23; 95% CI, 1-1.53), patients with metastatic disease vs. locoregional disease (OR = 1.63; 95% CI, 1.29-2.05) and patients who experienced COVID-19 complications vs. those who did not experience complications (OR = 1.52; 95% CI, 1.24-1.86).
Conversely, researchers observed a lower likelihood of cancer treatment delays among patients who reported residing in areas with a higher proportion of Hispanic or Latino residents (OR = 0.76; 95% CI, 0.6-0.95) and among those who contracted COVID-19 later during the pandemic (between January and March 2021) vs. those infected between March and June 2020 (OR = 0.38; 95% CI, 0.26-0.53).
Moreover, 47% of the 202 patients requiring radiation treatment had two or more comorbidities that appeared associated with delays in radiation treatment (OR = 2.69; 95% CI, 1.2-6.2), whereas patients with a higher local-area median household income had a lower likelihood for delays in radiation treatment (OR = 0.41; 95% CI, 0.17-0.94).
Among the 125 patients requiring surgery, 71% experienced delays in surgical treatment and researchers found that patients residing in the South had a much higher rate of delays than patients in the Midwest (OR = 9.66; 95% CI, 2.14-52.3). Of note, patients with two or more comorbidities experienced a lower likelihood of delays in surgery compared with those with one or no comorbidities (OR = 0.26; 95% CI, 0.07-0.88).
“These results show that various vulnerable populations experienced systematic cancer treatment delays and that a positive COVID-19 test may be one additional reason contributing to overall poor outcomes among these populations,” Mullangi told Healio. “Our findings are in line with other data that show persistent disparities in COVID-19-associated outcomes in subgroups of disadvantaged and minority populations, although other hypotheses for this have been advanced elsewhere, such as gaps in vaccination rates, spread of virus initially to urban areas, and infections being concentrated among essential workers who are disproportionately members of racial and ethnic minority communities.”
Investigators acknowledged study limitations, including the fact that the ASCO registry contains limited information about practice factors and the participating ASCO practices may not represent the general population. In addition, researchers only enrolled patients with positive COVID-19 test results and did not have information on patients with cancer but without COVID-19 treated at the same facilities.
“Three things would be logical next steps,” Mullangi said. “For one, the hope is that we can understand the near-term and medium-range outcomes of these treatment delays with longer follow-up. Two, with a larger sample size either with this registry or a different data source, there is a need to differentiate between patients who had one-time delays vs. persistent delays vs. treatment discontinuation due to spread of cancer, or loss of functional status of patient. Three, we need to better understand the impact of clinic-specific protocols, such as testing for routine surveillance and testing for symptoms on rates of COVID-19 detection and outcomes. However, we would only be able to do this with either practice identification or a separate study combining surveys of practice managers with these results.”
Samyukta Mullangi, MD, MBA, can be reached at smullangi13@gmail.com.

[ad_2]
Source link