












- By FYH News Team
[ad_1]
Question
Do disparities in Consumer Assessment of Healthcare Providers and Systems (CAHPS) exist between racial and ethnic groups with Alzheimer disease and related dementias (ADRD)?
Findings
In this cross-sectional study, significant racial and ethnic disparities in CAHPS score were observed according to the analysis of 568 368 community-based Medicare beneficiaries aged 65 years and older who were enrolled in an Accountable Care Organization. A proxy for social determinants of health explained 10% to 13% of CAHPS disparities.
Meaning
These findings suggest that it is imperative to implement targeted efforts to decrease disparities that could result in improvements in timely care and communication with clinicians for the aging diverse population with ADRD.
Importance
Consumer Assessment of Healthcare Providers and Systems (CAHPS) measures have been used widely to measure patient-centered care. Evidence is needed to understand CAHPS measures among racial and ethnic minority patients with Alzheimer disease and related dementias (ADRD).
Objective
To examine racial and ethnic disparities in CAHPS among patients with ADRD and to examine the association between social determinants of health and CAHPS disparities.
Design, Setting, and Participants
This study focused on patients with ADRD who were enrolled in Medicare Shared Savings Program Accountable Care Organizations (ACOs). The primary data sets were the 2017 Medicare Beneficiary Summary File and the beneficiary-level ACO data. The study population was limited to community-based beneficiaries who had a diagnosis of ADRD and were aged 65 years and older. Cross-sectional analyses and the decomposition approach were implemented. Data were analyzed from November 2021 to July 2022.
Exposure
Enrollment in a Medicare Shared Savings Program ACO.
Main Outcomes and Measures
Six ACO CAHPS measures were included: getting timely care, appointments, and information; how well providers communicate; patients’ rating of provider; access to specialists; health promotion and education; and shared decision-making. ACO CAHPS were continuous measures with possible ranges from 0 to 100. The summation of these 6 measures as an overall index was also created. In CAHPS measures, the term provider can include hospitals, home health care agencies, and doctors, among others.
Results
The final sample included 568 368 beneficiaries (347 783 female patients [61.2%]; 38 030 African American patients [6.69%], 6258 Asian patients [1.10%], 18 231 Hispanic patients [3.21%], and 505 849 White patients [89.0%]; mean [SD] age, 82.17 [7.95] years). Significant racial and ethnic disparities in CAHPS scores were observed. After controlling for beneficiary, hospital, and area characteristics, compared with their White counterparts, African American or Black (coefficient = −1.05; 95% CI, −1.15 to −0.95; P < .001), Asian (coefficient = −0.414; 95% CI, −0.623 to −0.205; P < .001), and Hispanic (coefficient = −0.099; 95% CI, −0.229 to 0.032; P = .14) patients with ADRD reported lower total CAHPS scores. Disparities were also observed among individual ACO CAHPS. Decomposition results showed that a proxy for social determinants of health explained 10% to 13% of disparities of ACO CAHPS between African American or Black vs White and Hispanic vs White patients with ADRD. Most of the racial and ethnic disparities, especially those between White and Asian individuals, could not be explained by the models used to analyze data.
Conclusions and Relevance
These results demonstrated significant variations in CAHPS by race and ethnicity among patients with ADRD enrolled in ACOs. Social determinants of health are critical in explaining racial and ethnic disparities. More research is needed to explain disparities in CAHPS.
It is estimated that there are more than 5 million US residents with Alzheimer disease and related dementias (ADRD) and that this number will increase to 13.9 million US residents by 2060.1 The incidence of dementia among Black and Hispanic older adults is approximately double and 1.5 times that of White older adults, respectively.2 The variation in ADRD risk is partly associated with differences in health conditions and socioeconomic status, among other factors for Black and Hispanic older adults relative to their White counterparts.3,4 Evaluation of patients’ (and their caregivers’) satisfaction and communication with health care clinicians is critical, especially for people with ADRD. For example, a patient’s trust in a clinician is linked with improved health behaviors.4 Often, health care clinicians develop this trust via communication (eg, relayed clear explanation, being an active listener), demonstrating care (eg, exhibiting intent to address their health condition), and showing competence (eg, having expertise, being methodical).5
Consumer Assessment of Healthcare Providers and Systems (CAHPS) measures have been used widely in the literature to measure this patient- centered, consumer-centered care through the patient experience. CAHPS surveys patient-physician communication, patient’s self-reported satisfaction with the clinicians, and shared decision-making. Lower CAHPS scores often reflected lack of health care access and lack of patient trust, and members of racial and ethnic minority groups were more likely to report poor patient experience (ie, lower CAHPS scores).6–10 CAHPS measures related to access to specialists, communication, educational information, timeliness, and shared decision-making are all substantial factors in the care experience of patients with ADRD and their caregivers.11
To our knowledge, this is the first study to examine CAHPS measures among patients with ADRD and associated racial and ethnic disparities. We hypothesized that patients with ADRD belonging to racial and ethnic minority groups, on average, scored lower on CAHPS than their White counterparts. Social determinants of health (SDOH) have been constantly identified as one of the main barriers to quality health care.12 Physicians caring for Hispanic patients found challenges in delivering high-quality care for several reasons, including obstacles with communication.13 Patients with limited English ability may encounter barriers when attempting to engage.14 Separately, factors such as cultural preferences may impact the ideal care setting for persons with ADRD.15 Hence, we further hypothesized that the differences between CAHPS by race and ethnicity, if any, might reflect variations of SDOH and cultural preferences.
This cross-sectional analysis followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. The study was approved by the University of Maryland institutional review board. The requirement for informed consent was waived because the study used secondary data analysis. Our study focused on patients with ADRD who were enrolled in Medicare Shared Savings Program (MSSP) Accountable Care Organizations (ACOs). Approximately 37% of Medicare enrollees with ADRD participated in an ACO in 2017.16 Beneficiaries receiving care from ACOs, relative to non-ACO enrollees, had better experiences with access to care and care coordination.17 Our study focused on this fairly homogeneous population given the data availability, and we speculated that the racial and ethnic disparities might be more pronounced among the entire aging ADRD population.
According to the National Institute on Minority Health and Health Disparities framework, our study included measures at multilevels. The primary data sets of the study were the 2017 Centers for Medicare and Medicaid Services Medicare Beneficiary Summary File (CMS MBSF). To capture ACO characteristics, we further linked the CMS MBSF with the 2017 MSSP ACO data. Specifically, using the ACO identifiers, we were able to capture the ACO CAHPS evaluations reported by the CMS 2017 ACO Quality Reporting Documentation.18 Finally, we merged our data with the 2017 American Community Survey and the Area Health Resource File using beneficiaries’ zip codes and county identifications.
Our study focused on patients with a diagnosis of ADRD using the CMS Chronic Conditions Data Warehouse measure. The sample was limited to community-based fee-for-service (at least 12 months) beneficiaries aged 65 years and older. Medicare Advantage and dual-eligible beneficiaries were excluded from the analysis. Patients were linked to the ACO beneficiary level file shared savings program.
Our study focused on ACO CAHPS measures endorsed by the National Quality Forum. The CAHPS survey assesses the outcome of ACOs on patient as well as caregiver experiences. Specifically, ACO CAHPS includes, but is not limited to, an analysis of the patient’s experience with care coordination, use of specialists, shared decision-making, and health education. CAHPS survey data can be found on the Care Compare and are used by the Quality Payment Program.18
In the main results, we report our findings using CAHPS indicators as continuous variables to capture the variations in the scores. Six ACO CAHPS measures were included: Getting Timely Care, Appointments, and Information (ACO1); How Well Your Providers Communicate (ACO2); Patients’ Rating of Provider (ACO3); Access to Specialists (ACO4); Health Promotion and Education (ACO5); and Shared Decision-Making (ACO6). ACO1 through ACO6 were continuous measures with possible ranges from 0 to 100. We created the summation of these 6 measures as an overall index.
The key independent variable in this study was the Research Triangle Institute Race Code. The variable includes the following racial and ethnic groups: African American or Black (Black), Asian or Pacific Islander (Asian), Hispanic or Latinx (Hispanic), and non-Hispanic White (White). We included several covariates, controlling for age, sex, and health. We also accounted for a range of health indicators, common coexisting chronic conditions for ADRD, obtained from the MBSF using the Chronic Conditions Data Warehouse: acute myocardial infarction, asthma, atrial fibrillation, heart failure, chronic obstructive pulmonary disease, depression, diabetes, hyperlipidemia, hypertension, and stroke or transient ischemic attack.19
We included SDOH measures in the analysis. Consistent with the literature on ADRD, we included zip code level percentages of residents with high school degrees and higher, living in poverty, and who were African American or Black.20 We also included the indicator of whether the whole county was a mental health shortage area. State indicators were included in the main analysis. Alternatively, we also used the Area Deprivation Index (ADI) as an overall indicator of the SDOH of the area.21 ADI allows for rankings of neighborhoods by socioeconomic disadvantages in a region, considering the domains of income, education, employment, and housing quality. ADI has been used to inform health policy design for disadvantaged neighborhood groups.22 We created an index if the ADI score of beneficiaries’ zip codes was higher than the ADI national rank of 50%, indicating persons residing in socioeconomically challenged neighborhoods.
Analysis for this study was at the beneficiary level. We first compared the ACO CAHPS measures, characteristics of beneficiaries, and SDOH by race and ethnicity. We used the ordinary least square regression to estimate the variation of ACO CAHPS measures by race and ethnicity. We first reported the regression results only controlling for beneficiaries’ demographic and health indicators (model 1). Then, we expanded model 1 by applying the state-fixed effect ordinary least square estimation and controlling for measures of SDOH (model 2). We applied the full model (model 2) to examine the overall ACO CAHPS (the summation) score as well as each individual ACO CAHPS score (ACO1-ACO6).
We were interested in understanding whether our models with the beneficiary and area-level measures could explain racial and ethnic disparities in ACO CAHPS. To do this, we applied the Blinder-Oaxaca decomposition model.23–26 The Blinder-Oaxaca decomposition model is a regression-based model. For example, to decompose the difference in the ACO CAHPS score between Black and White patients with ADRD, ordinary least square regressions of these 2 groups were estimated separately. These 2 estimations were then rearranged to indicate (1) the portion of the difference due to observed characteristics (ie, all of the control variables), and (2) the portion of the difference due to unobserved heterogeneities, such as cultural background and discrimination. Among the observed population characteristics, disparities associated with each specific factor, such as SDOH, were quantified. Similar approaches were applied to study the disparities of ACO CAHPS between White and other racial and ethnic groups.
We implemented sensitivity analyses to test the robustness of our study. We created binary variables for each of these 6 measures, which equaled 1 if the ACO CAHPS (ACO1-ACO6) measure was above the 75th percentile (ie, the highest [best] top 25th percentile). Furthermore, we created a composite ACO CAHPS of 1 if any of the 6 ACOs exceeded the 25th highest percentile. We reported these findings in the eFigure and eTable in the Supplement. Results were consistent with our main findings.
STATA statistical software version 17 MP4 (StataCorp) was used to analyze the data. Statistical analysis was done with 2-sided hypothesis tests, including χ2 tests for categorical variables, analysis of variance tests for continuous variables, t tests for the mean differences by each race and ethnicity group, and ordinary least square (OLS) regression to estimate the variation of ACO CAHPS measures by race and ethnicity. The statistical significance was set at P < .05. The analysis was implemented from November 1, 2021, to July 29, 2022.
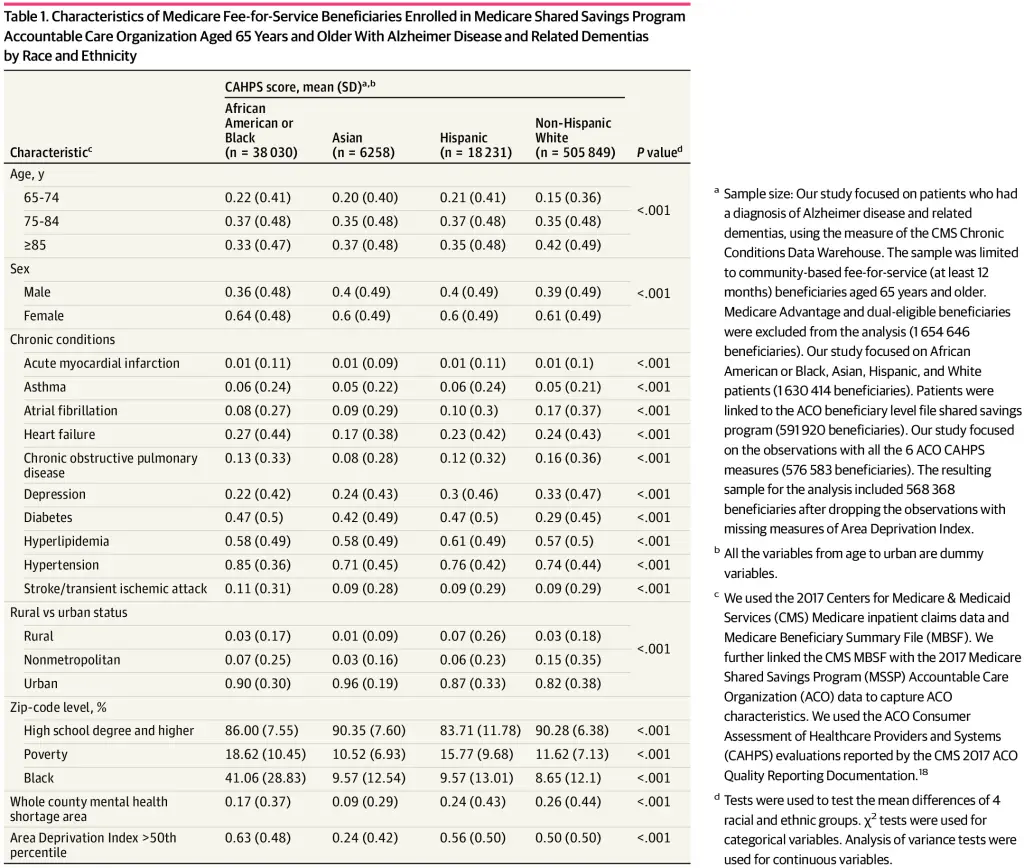
The final sample included 568 368 beneficiaries (347 783 female patients [61.2%]; 38 030 African American patients [6.69%], 6258 Asian patients [1.10%], 18 231 Hispanic patients [3.21%], and 505 849 White patients [89.0%]; mean [SD] age, 82.17 [7.95] years). Rates of diabetes were substantially higher among African American or Black, Asian and Hispanic populations than White counterparts. Other racial groups were more likely to live in urban areas than White patients. African American or Black and Hispanic patients with ADRD were also more likely to live in areas with lower education, higher poverty rates, and mental health shortage areas. Full demographic information is available in Table 1.
The comparison of the ACO CAHPS scores by race and ethnicity among Medicare fee-for-service beneficiaries aged 65 years and older are presented in Table 2. Results showed that White patients reported higher ACO CAHPS total score, and higher CAHPS scores on receiving timely care (ACO1), provider communication (ACO2), patients’ rating (ACO3), and access to specialists (ACO4), compared with African American or Black, Asian, and Hispanic patients with ADRD. Compared with White beneficiaries, Hispanic beneficiaries reported higher scores on health promotion (ACO5), and Asian and Hispanic beneficiaries reported higher scores on shared decision-making (ACO6).
After controlling for characteristics of beneficiary demographic and health indicators, model 1 showed significant racial and ethnic disparities in enrolling in ACOs with high ACO CAHPS scores (Table 3). Disparities between African American or Black patients (coefficient = -1.051; 95% CI, −1.15 to -0.95; P < .001) and White patients (coefficient = −0.414; 95% CI, −0.623 to −0.205; P < .001) and Asian patients (coefficient = −0.099; 95% CI, −0.229 to 0.032; P = .14) and White patients remain after controlling for SDOH and applying state-fixed effects (model 2). Disparities of the CAHPS total score between Hispanic and White individuals became insignificant. Results also showed that compared with urban residents, residents in rural and nonmetropolitan areas were less likely to enroll in ACOs with high CAHPS scores. Residents in areas with low education, higher poverty rate, a higher African American or Black population, and mental health shortage areas were also less likely to enroll in ACOs with high CAHPS scores.
Similarly, disparities were observed among individual CAHPS measures of getting timely care, provider communication, and patient’s rating (Table 4). African American or Black and Asian patients reported lower access to specialties, and African American or Black patients reported a lower rate of shared decision-making, compared with White patients. Compared with White beneficiaries, African American or Black and Hispanic patients reported higher CAHPS scores on health promotion and education, and Asian patients reported higher scores on shared decision-making. To facilitate the interpretation, in the eTable in the Supplement, we reported the results of the logistic regressions and tested the likelihood of enrolling in the ACOs with the top 25th percentile of each CAHPS score. Marginal effects were reported. Results were similar. Compared with White patients, African American or Black patients were less likely to enroll in the ACOs with the top scores of ACO1 through ACO6.
Results of the decomposition analyses estimated higher CAHPS total scores for White patients. Our empirical model explained a substantial part of racial and ethnic disparities (ie, 18% of African American or Black vs White, and 14% of Hispanic vs White) of CAHPS. Meanwhile, the results suggested the majority of disparities (82%-86%) could not be explained by our models. Among all the controlled variations, the ADI was the most substantial factor, which explained 13% and 11% of disparities between African American or Black vs White and Hispanic vs White patients with ADRD, respectively. Our model specification, however, could not explain disparities of CAHPS scores among Asian vs White patients with ADRD. Results showed that if all the controlled variables were the same between Asian and White patients, Asian patients were supposed to report higher CAHPS scores (ie, the negative explained score in Table 5).
The findings of this cross-sectional study demonstrated significant racial and ethnic disparities in CAHPS scores. The results also showed that the ADI, an indicator of SDOH, explained 10% to 13% of disparities of ACO CAHPS between African American or Black vs White and Hispanic vs White patients with ADRD. Most of the racial and ethnic disparities, especially the disparities between Asian and White patients, could not be explained by beneficiaries’ demographic characteristics, coexisting health conditions, and the ADI. Our results support the literature that patients with ADRD belonging to racial and ethnic minority groups encountered worse quality uncoordinated health care, including a lack of well-timed access to primary care. Our assessment of ADI demonstrated the link between SDOH and existing health disparities. It is also possible that some disparities were tied to cultural preferences, availability of caregivers, biases, and other factors that were not measured using the existing data sets.
Racial and ethnic minority patients with ADRD reported lower CAHPS on getting timely care. Evidence suggests that minority populations are more likely to have later-stage diagnoses, experience delays in timely primary care, and lack access to coordinated care.3,4,27 Access to timely care may prevent disease progression. Results also suggested African American or Black patients reported lower CAHPS scores on communication, rating, access to specialties, and shared decision-making. Prompt communication between the person with dementia, their caregiver, and the team of health care clinicians is one of the critical factors in successful transitions in care.28 Taking a person-centered approach to care transitions has the potential to improve the quality of care provided—delivering person-centered care involves accounting for patients’ preferences while also considering the caregiver throughout the process.
Results showed encouraging findings on health promotion and education. African American or Black and Hispanic patients reported higher scores than White cohorts. Racial and ethnic minority groups, immigrants, persons with low socioeconomic status, and those with low self-reported health on average have a lower level of patient activation relative to their counterparts.1 We speculated that the ACO enrollment might have played a role in promoting health education, especially among African American or Black and Hispanic patients and their caregivers. It will be interesting to explore the different characteristics of health care clinicians that serve these minority patients. These clinicians might share their experience of effectively engaging minority patients with ADRD and their caregivers. We speculated that cultural competency training, language, and clinician-patient racial and cultural concordance might be critical.
Our study also found that SDOH ADI was associated with ACO CAHPS, indicating the need for targeted approaches to address SDOH. Several SDOH are associated with cognition and ADRD diagnosis, such as low socioeconomic status, low levels of education, economically disadvantaged regions with limited physical resources, and food security, among other factors.3,29 Results of our study suggested that ACOs aimed at improving access to necessary, timely care may help decrease existing disparities. Resources can be directed toward SDOH to improve the well-being of older adults. Our findings were also consistent with the structural racism and discrimination (SRD) literature and supported the framework of SRD patients with ADRD30–34. The components of SRD, such as institutional racism, systemic barriers, and other health determinants, are key factors to target to decrease disparities. In addition, the present study is the first, to our knowledge, to measure the SRD at the intermediary level (ie, physician-patient interaction) for the ADRD population.
Our findings suggested that there are substantial rural and urban disparities in enrollment of beneficiaries in ACOs with high CAHPS. Often, rural regions have fewer resources than urban areas. Variations in the availability of health care services between rural and urban regions may affect timely access to care. One study35 found that older Medicare fee-for-servicebeneficiaries in rural areas are potentially underdiagnosed with ADRD and receive delayed diagnosis.
Given our growing diverse population of older adults, it is imperative that future research reflects their care experiences and needs. For example, given the lack of research on older Asian American adults, we are limited in our ability to fully explain the disparities in our study. From the literature on the aging Asian immigrants receiving care for depression, we speculated that implementing a patient-centered model in decision-making could lead to the positive engagement of the individual.
Our study had several limitations. First, our model used multilevel controls according to the National Institute on Minority Health and Health Disparities framework but still might have missed other variables, such as the severity of the diseases, and other factors missing in the claims data, such as measures reflecting preferences, caregiver availability, and burdens, among others. Second, our study focused on MSSP ACO enrollees. Results should not be applied to the general aging population. Although the study population was homogeneous, we were able to observe significant variation among individuals belonging to different racial and ethnic groups. According to the literature, ACO enrollment might be associated with racial disparities, and White individuals were overrepresented. It is also possible that people not enrolled in an ACO experience a lower quality of care and worse disparities. Future studies may improve the data collection of the CAHPS measures to facilitate the assessment of the aging population. Additionally, our study documented CAHPS variation among patients with ADRD of different races and ethnicities. Future studies may further investigate modifiable factors that can be used to reduce observed disparities. It is a teachable moment to promote health equity and to use the opportunities of ongoing policy initiatives such as reimbursement and improving health infrastructure.
The burden of ADRD in the US will become increasingly high as the aging population grows and racial and ethnic diversity increases. CAHPS measures have been used widely to measure patient-centered care. It is also a proxy measure of intermediary determinants (ie, the interpersonal experience) of SRD. Our results demonstrated significant variations in CAHPS by race and ethnicity among patients with ADRD. Results suggested the urgent need to understand the factors that contributed to such disparities. Policy initiatives targeting the structural factors, such as payment reform and care coordination, might be useful to improve CAHPS for racial and ethnic minority patients with ADRD, a population that has faced SRD during their life courses.
Accepted for Publication: August 9, 2022.
Published: September 27, 2022. doi:10.1001/jamanetworkopen.2022.33436
Open Access: This is an open access article distributed under the terms of the CC-BY License. © 2022 Albaroudi A et al. JAMA Network Open.
Corresponding Author: Jie Chen, PhD, Department of Health Policy and Management, School of Public Health, University of Maryland, 4200 Valley Dr, 3310E School of Public Health Building, College Park, MD 20742 (jichen@umd.edu).
Author Contributions: Dr Chen had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Both authors.
Acquisition, analysis, or interpretation of data: Chen.
Drafting of the manuscript: Both authors.
Critical revision of the manuscript for important intellectual content: Both authors.
Statistical analysis: Chen.
Obtained funding: Chen.
Administrative, technical, or material support: Both authors.
Supervision: Chen.
Conflict of Interest Disclosures: Ms Albaroudi reported working for the Medicaid and CHIP Payment and Access Commission outside the submitted work. No other disclosures were reported.
Funding/Support: This study is supported by the National Institute on Aging (grant R01AG62315-01A1 to Dr Chen) and the National Institute on Minority Health and Health Disparities (R01MD011523S1 to Dr Chen).
Role of the Funder/Sponsor: The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Meeting Presentation: The study was presented at the poster session of the Alzheimer’s Association International Conference; Tuesday, August 2, 2022; San Diego, California, and online.
Additional Contributions: Minqi Wang, PhD (University of Maryland), built the analytic data file and received no compensation beyond their normal salary.
KA, Xu
W, Gaglioti
AH,
et al. Racial and ethnic estimates of Alzheimer’s disease and related dementias in the United States (2015-2060) in adults aged ≥65 years. Alzheimers Dement. 2019;15(1):17-24. doi:10.1016/j.jalz.2018.06.3063PubMedGoogle ScholarCrossref
AR, Kaye
J, Allore
HG, Botoseneanu
A, Thielke
SM. An agenda for addressing multimorbidity and racial and ethnic disparities in Alzheimer’s disease and related dementia. Am J Alzheimers Dis Other Demen. 2020;35:1533317520960874. doi:10.1177/1533317520960874PubMedGoogle ScholarCrossref
JH, Greene
J, Shi
Y, Mittler
J, Scanlon
D. Taking the long view: how well do patient activation scores predict outcomes four years later? Med Care Res Rev. 2015;72(3):324-337. doi:10.1177/1077558715573871PubMedGoogle ScholarCrossref
CA, Elliott
MN, Haviland
AM,
et al. Experiences of care among Medicare beneficiaries with ESRD: Medicare Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey results. Am J Kidney Dis. 2013;61(3):440-449. doi:10.1053/j.ajkd.2012.10.009PubMedGoogle ScholarCrossref
AJ, Toledo
G, Ochoa
CY, Hamilton
AS. Racial/ethnic disparities in patient experiences with health care in association with earlier stage at colorectal cancer diagnosis: findings from the SEER-CAHPS data. Med Care. 2021;59(4):295-303. doi:10.1097/MLR.0000000000001514PubMedGoogle ScholarCrossref
JM, Riffin
C, Havyer
RD,
et al. Integrating family caregivers of people with Alzheimer’s Disease and dementias into clinical appointments: identifying potential best practices. J Appl Gerontol. 2020;39(11):1184-1194. doi:10.1177/0733464819880449PubMedGoogle ScholarCrossref
KL, Dardess
P, Maurer
M,
et al. Patient and family engagement: a framework for understanding the elements and developing interventions and policies. Health Aff (Millwood). 2013;32(2):223-231. doi:10.1377/hlthaff.2012.1133PubMedGoogle ScholarCrossref
S, Chen
J. Racial and ethnic patterns and differences in health care expenditures among Medicare beneficiaries with and without cognitive deficits or Alzheimer’s disease and related dementias. BMC Geriatr. 2020;20(1):482. doi:10.1186/s12877-020-01888-yPubMedGoogle ScholarCrossref
J. Accountable care organizations and racial and ethnic disparities among patients with Alzheimer’s and related dementia diseases: public health: engaging people in ADRD research. Alzheimers Dement. 2020;16(S10):e043283. doi:10.1002/alz.043283Google ScholarCrossref
AM, Malone
DC, Warholak
TL, Armstrong
EP. Health disparities in cost of care in patients with Alzheimer’s disease: an analysis across 4 state Medicaid populations. Am J Alzheimers Dis Other Demen. 2013;28(1):84-92. doi:10.1177/1533317512467679PubMedGoogle ScholarCrossref
EL, Jicha
GA, Christian
WJ, Schreurs
BG. Rural-urban differences in Alzheimer’s Disease and related disorders diagnostic prevalence in Kentucky and West Virginia. J Rural Health. 2016;32(3):314-320. doi:10.1111/jrh.12155PubMedGoogle ScholarCrossref
[ad_2]
Source link
Trending Topics
Features
- Drive Toolkit
Download and distribute powerful vaccination QI resources for your community.
- Health Champions
Sign up now to support health equity and sustainable health outcomes in your community.
- Cancer Early Detection
MCED tests use a simple blood draw to screen for many kinds of cancer at once.
- PR
FYHN is a bridge connecting health information providers to BIPOC communities in a trusted environment.
- Medicare
Discover an honest look at our Medicare system.
- Alliance for Representative Clinical Trials
ARC was launched to create a network of community clinicians to diversify and bring clinical trials to communities of color and other communities that have been underrepresented.
- Reducing Patient Risk
The single most important purpose of our healthcare system is to reduce patient risk for an acute event.
- FYH News Team
- Subash Kafle
- Subash Kafle



