February 02, 2023
3 min read
[ad_1]
February 02, 2023
3 min read
![]()
Eckhert E, et al. JAMA Oncol. 2023;doi:10.1001/jamaoncol.2022.7146.
Disclosures:
The Biostatistics Shared Resource of the NIH-funded Stanford Cancer Institute, BRCA Foundation, Breast Cancer Research Foundation, Jan Weimer Junior Faculty Chair in Breast Oncology, Regents of the University of California’s California Breast Cancer Research Program, Susan and Richard Levy Gift Fund, and Suzanne Pride Bryan Fund for Breast Cancer Research supported the study. Eckhert reports no relevant financial disclosures. Please see the study for all other authors’ relevant financial disclosures.
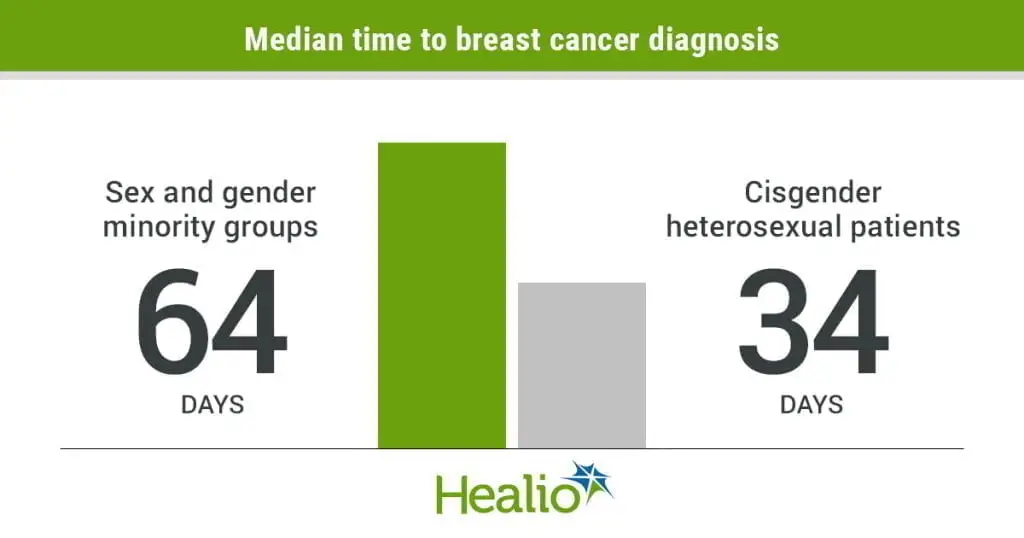
Members of sex and gender minority groups experienced longer times from symptom onset to breast cancer diagnosis compared with a cohort of cisgender heterosexuals, according to study results published in JAMA Oncology.
Additionally, sex and gender minority individuals appeared more likely to decline oncologist-recommended treatment and experienced higher rates of recurrence, researchers noted.

“This project was prompted by my prior research in LGBTQ+ health disparities, as well as by my time spent designing and teaching the Stanford Internal Medicine LGBTQ Health Curriculum for resident physicians,” Erik Eckhert, MD, MS, postdoctoral fellow in hematology and oncology at Stanford University Hospital, told Healio. “From these experiences, I came to understand that our health care apparatus is primarily designed by and for cisgender heterosexual people. As a corollary, LGBTQ+ people are often discriminated against in health care settings or have difficulty finding a provider who is knowledgeable about caring for populations of sex and gender minority groups.”

Erik Eckhert
Eckhert said that although the qualitative oncology literature is “replete with LGBTQ+ patient-reported experiences of subtle to overt discrimination,” high-quality quantitative data on health outcomes for LGBTQ+ people with breast cancer are lacking.
“High-quality data are necessary to obtain buy-in from major players in the larger health care system to address the health care disparities that LGBTQ+ patients have been telling us about for years,” he said. “With that in mind, I sought to harness the power of the Oncoshare database created by Allison W. Kurian, MD, MSc, which integrates the data of patients with breast cancer across the Stanford and Sutter health care systems with the California Cancer Registry, to characterize health disparities for patients from sex and gender minority groups with breast cancer.”
Investigators evaluated the quality of breast cancer treatment and recurrence outcomes among 92 patients (78.3% white; 80% lesbian; 13% bisexual; 6% transgender) with breast cancer from sex and gender minority groups receiving treatment at an academic medical center between Jan. 1, 2008, and Jan. 1, 2022. They matched those individuals with 92 cisgender heterosexual patients (63% white) with breast cancer. Median age at diagnosis among all patients was 49 years.
Main outcomes included patient demographic and clinical characteristics, treatment quality, appropriate referral for genetic counseling and testing, mastectomy vs. lumpectomy, receipt of chest reconstruction, adjuvant radiation therapy after lumpectomy, neoadjuvant chemotherapy for stage III breast cancer, antiestrogen therapy for at least 5 years for ER-positive disease, ERBB2-directed therapy for ERBB2-positive disease, patient refusal of an oncologist-recommended treatment, time from symptom onset to tissue diagnosis, time from diagnosis to first treatment and time from breast cancer diagnosis to first recurrence.
Researchers hypothesized that patients from sex and gender minority groups have disparities in one or more quality metrics compared with cisgender heterosexual patients.
Results showed patients from sex and gender minority groups experienced delays in time from symptom onset to breast cancer diagnosis compared with the cisgender heterosexual cohort (median time to diagnosis, 64 vs. 34 days; multivariable adjusted HR = 0.65; 95% CI, 0.42-0.99).
Moreover, patients from sex and gender minority groups appeared more likely to decline an oncologist-recommended treatment modality (38% vs. 20%; multivariable adjusted OR = 2.27; 95% CI, 1.09-4.74) and more likely to experience breast cancer recurrence (multivariable adjusted HR = 3.07; 95% CI, 1.56-6.03).
Limitations of the study included the observational and retrospective design, the imbalance of race/ethnicity between the two groups, and the fact that sex and gender minority research is always subject to selection bias because patients who choose to disclose their sexual orientation to their care teams and to researchers tend to have greater social resources than those who do not, researchers noted.
The findings have two major implications, which should also be next steps for research, Eckhert told Healio.
“The first step is to initiate the addition of sexual orientation and gender identity [SOGI] data to national and state cancer databases,” he said. “This data is not routinely collected on a large scale and is the only way for oncologists to get a better scope of the problems facing sex and gender minority populations. Concurrently, there needs to be better provider training in LGBTQ health so that providers are more knowledgeable about how to approach and care for sex and gender minority populations.”
Erik Eckhert, MD, MS, can be reached at eckhert@stanford.edu.
[ad_2]
Source link